Staphylococcus
There are 2 types of gram-positive cocci bacteria. These are Staphylococci and streptococci as highlighted below. Staph bacteria are catalase-positive. The most important staphylococcus is staph aureus which is coagulase-positive in addition to being catalase positive. Coagulase-negative staph bacteria are staph epidermidis and staph saprophyticus.
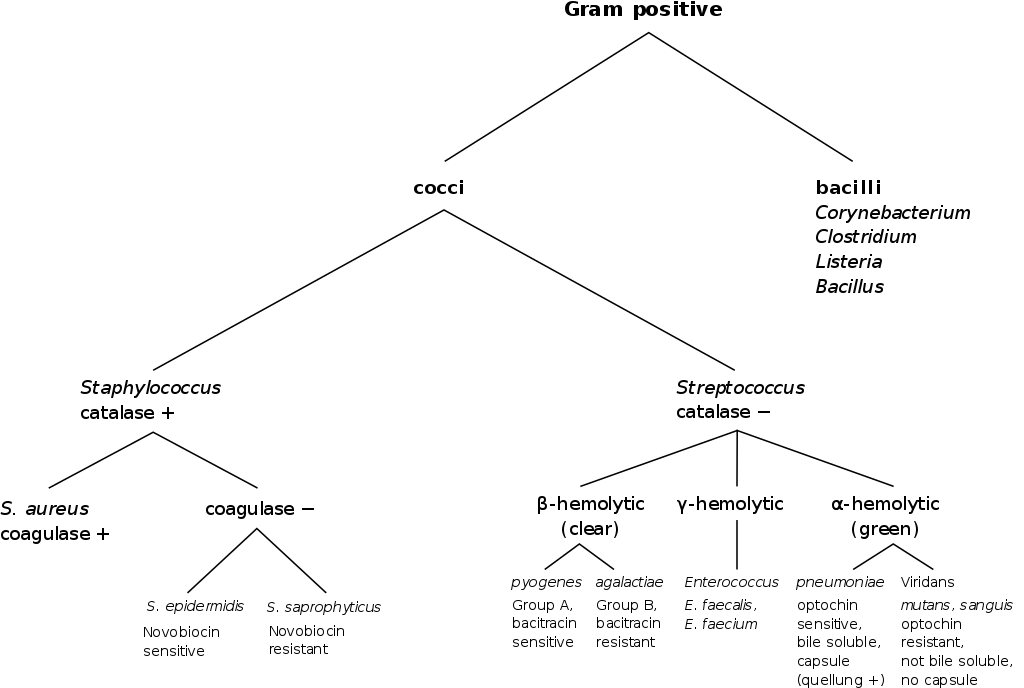 Diagram 1. All 3 Staphylococci discussed below and how to identify them
Diagram 1. All 3 Staphylococci discussed below and how to identify them
Staph aureus
S. aureus lives mostly in the noses of 30% of people benignly and produces a yellow pigment (aureus=golden). This bacteria s also beta-hemolytic. Coagulase test helps tell this bacteria apart from the other types of staphylococci. The presence of S. aureus in the blood will result in coagulation and the formation of fibrin clots. This bacteria also produce protein A virulence factor which helps it to prevent phagocytosis. Staph bacteremia can often be caused by unsterile central lines in very sick patients. Infection with S. aureus can cause the following conditions:
- Toxic shock syndrome
- S. aureus produces a toxin called TSST-1
- This toxin gets in the blood and causes bacteremia
- Classically a result of staph infection and packing (tampons, wound packing)
- Symptoms
- Fever
- Shock
- Diarrhea
- Sunburn like rash=erythroderma
- The skin of palms and soles of feet detaches
- Multi-organ failure
- Food poisoning
- Food contaminated from someone's nose
- Bacteria grow at room temperature and produces the enterotoxin
- Mayonnaise is a commonly affected food
- Symptoms
- Nausea, abdominal cramps, vomiting
- 3-6 hours later
- Scalded skin syndrome
- Caused by exfoliatin protein produced by S. aureus
- Occurs in newborns at 3-7 days
- Symptoms
- Fever
- Diffuse rash starting from the mouth
- Skin detaches due to intraepidermal skin damage
- Nikolsky's sign
- Skin infections
- Impetigo
- Impetigo usually caused by group A strep or S. aureus.
- Yellow-colored with crusts

- Bullous impetigo
- Bullous impetigo is caused y S. aureus
- Fluid-filled blister-like lesions
- Common in children
- Impetigo
- Pneumonia
- Lobar pneumonia cause
- Post-infectious
- Usually after influenza
- Endocarditis
- Acute endocarditis
- Even in patients who have healthy valves
- This is different from the subacute version
- Subacute version is caused by strep viridans
- This also requires a history of valvular disease
- Osteomyelitis
- Usually in the spine for adults, long bones for pediatric patients
- Imaging can diagnose this condition
- Symptoms
- Fever
- Localized pain
- Abscesses
- Skin and tonsils
- Lesions filled with pus
- In the skin
- Furuncle = boil = infection of a hair follicle
- Carbuncle = multiple boils together
- May require incision and drainage as these lesions are walled off (antibiotic inaccessible)
- Meningitis
- Cellulitis
- Mostly caused by beta-hemolytic streptococci
- S. aureus can also get into the deeper layers of skin and subcutaneous fat

Treatment
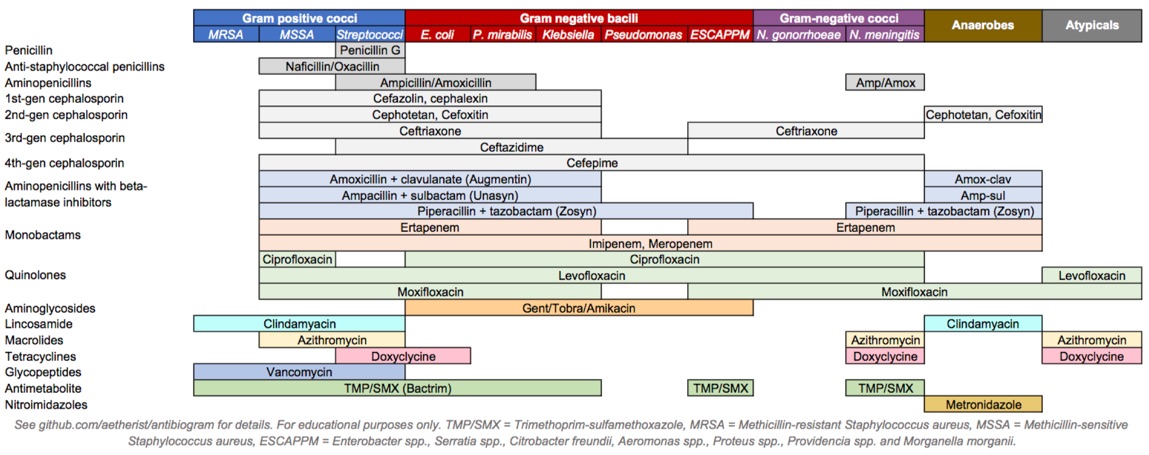
Diagram 2. Various antibiotics and their coverage.
Most strains are resistant to penicillins due to the production of beta-lactamases. There are some penicillins (namely, Naficilin and Oxacillin) that are effective with S. aureus. First-generation cephalosporins such as Cefalozin and Cephalexin are very effective towards this bacteria. Finally, beta-lactamase inhibitors can be administered along with beta-lactam antibiotics. Amoxicillin with clavulanate, Ampacilin with subactam, and Pipercilin with tazobactam are such combination agents that are effective in treating S. aureus.
Methicillin-resistant Staphylococcus aureus (MRSA)
These are strains of S. aureus that are resistant to beta-lactam antibiotics due to their modified penicillin-binding proteins. This makes them difficult to treat. In patients with MRSA or suspected MRSA, Vancomycin and daptomycin are the antibiotics used.
Staph Epidermidis
This catalase-positive and coagulase-negative staphylococcus is part of the normal skin flora of humans and normally does not cause any infection. However, this organism can play a role in contaminating blood samples. Oftentimes, multiple vials of blood are taken and cultured separately to avoid a false bacteremia diagnosis with S. epidermidis. Prosthetic materials in the blood can also be infected by this organism. This includes catheters, prosthetic body parts, and pacemakers.
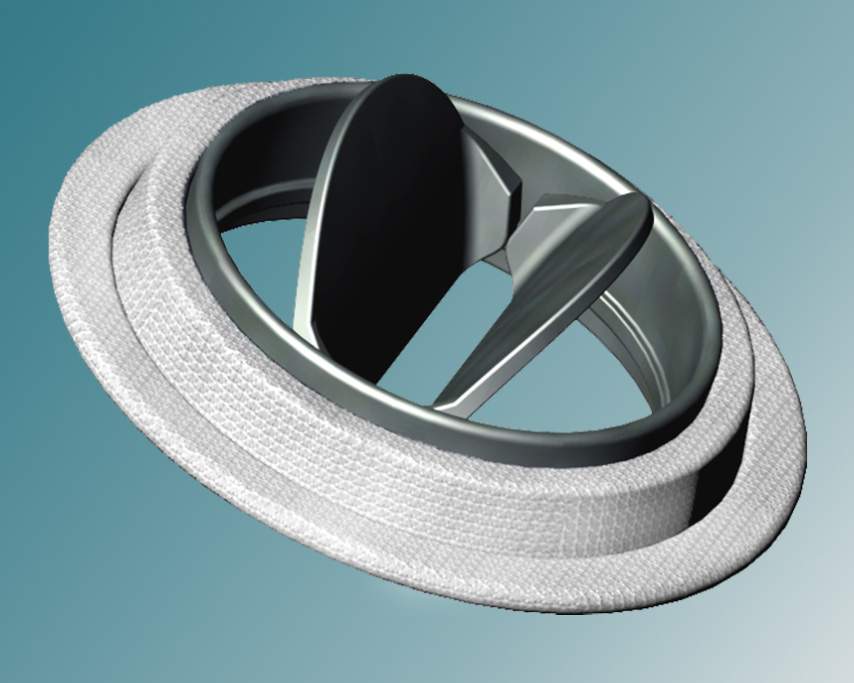
Picture 1. Prosthetic heart valves can be infected by staph epidermidis.
Treatment
This bacteria is usually methicillin-resistant and will not be affected by beta-lactam antibiotics. Just like MRSA, Vancomycin can be used for this type of infection.
Staph Saprophyticus
Although most cases of UTIs are caused by E.coli (as well as Proteus and Klebsiella) S. Saprophyticus can be a common cause of UTIs in sexually active females. Most cases occur within 24 hours of having sex and are known as "honeymoon cystitis". During sexual activity, this organism is displaced from normal vaginal and perineal flora into the female urethra. On urinalysis, the sample will be nitrite negative (E.coli will be nitrite positive).
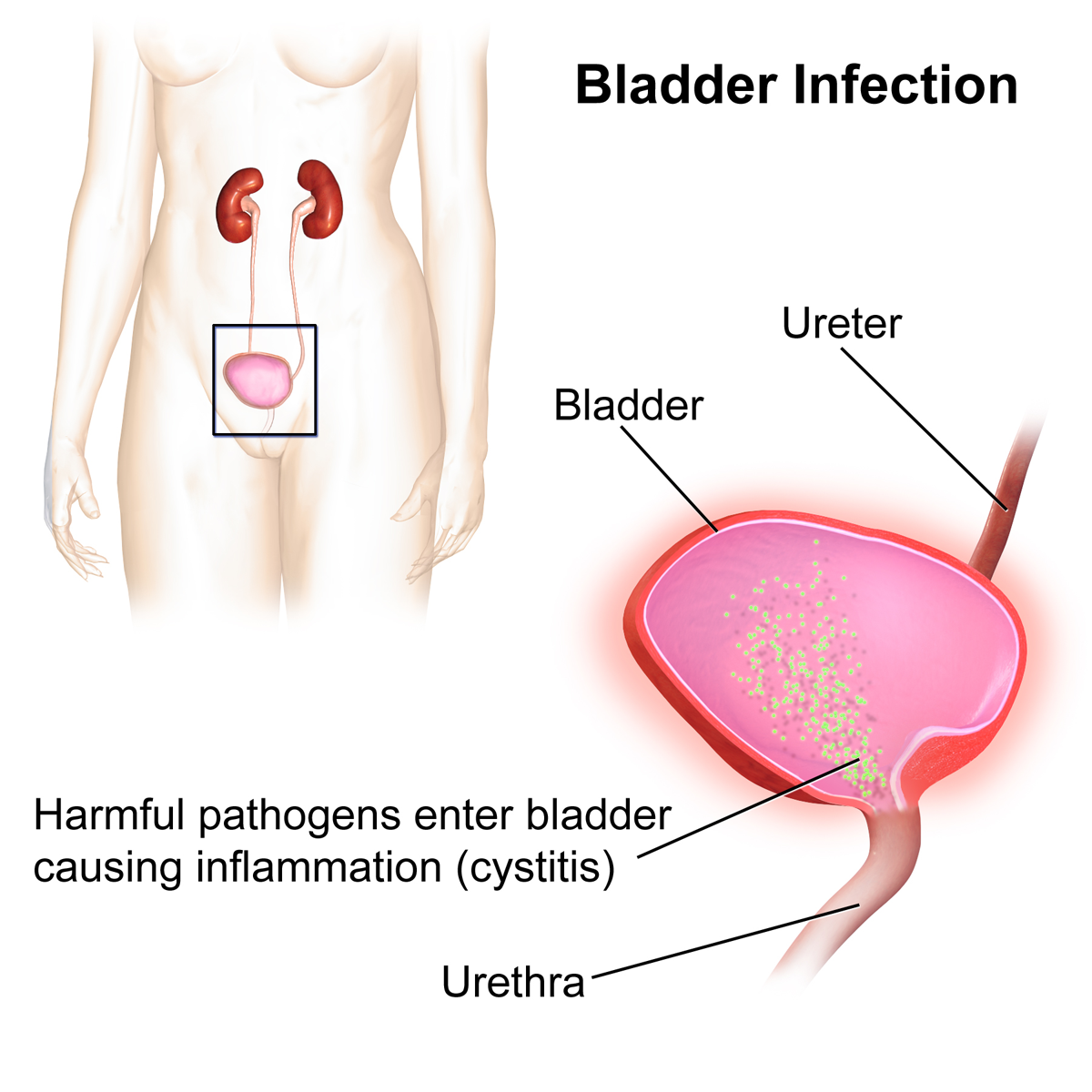
Picture 2. Females are susceptible to UTIs because of their short urethra, compared to males.
Treatment
Treatment is usually done with trimethoprim-sulfamethoxazole, a quinolone, or nitrofurantoin.
All information provided on this website is for educational purposes and does not constitute any medical advice. Please speak to you doctor before changing your diet, activity or medications.
