Urinary incontinence
Urinary incontinence is the involuntary leakage of urine from the bladder. This eventually leads to physical and emotional distress in the patient. This problem is especially prevalent in women during their lifetime, affecting about 30% above age 60.
Diagnosis
- History
- Assess severity of symptoms and medication use (rule out transient urinary incontinence)
- Physical exam
- Rule out functional causes (dementia, mobility problems, constipation)
- Ask the patient to cough or laugh to asses for stress incontinence
- Urinalysis and urine culture
- Rule out UTIs

- Ultrasound residual urine volume measurement
- Rule out urinary retention (normal residual urine < 100ml)

- Urinary diary
- >7 episodes of urination = frequency problem
- Can be variable depending on patient and habits
- Urodynamics
- Cystometry
- Involves filling up the bladder with sterile water
- Normally sensation to void occurs at >150ml and total bladder capacity is between 400-600ml
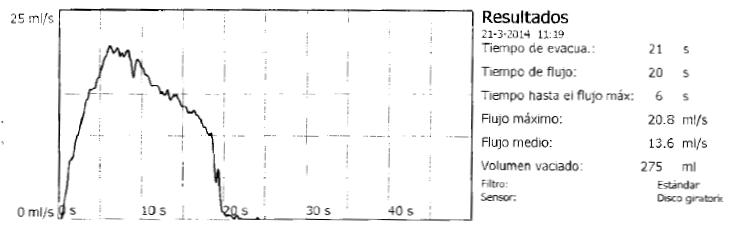
- Uroflowmetry
- Measures urinary flow rate and flow time
- Complex urodynamic testing
- Measures intravesical and intraabdominal pressures
- Cystometry
Classification
- Stress urinary incontinence (SUI)
- Mechanism
- Coughing, laughing, sneezing and other physical movements increase the intraabdominal pressure
- Increased abdominal pressure leads to increased bladder pressures, resulting in incontinence
- Causes
- Weakened pelvic floor due to pregnancy, menopause and trauma
- Diagnosis
- History consistent with SUI and physical exam demonstrating urinary incontinence
- Treatment
- Surgical
- Anterior colporrhaphy
- Not very durable over the long term
- Tension-free transvaginal tape
- New gold standard
- Minimally invasive
- Burch colposuspension
- Sutures placed at the Cooper ligament
- Collagen periurethral injections
- Collagen injected around the urethra and bladder neck for stress incontinence
- Anterior colporrhaphy
- Non-surgical
- Pelvic muscle exercises
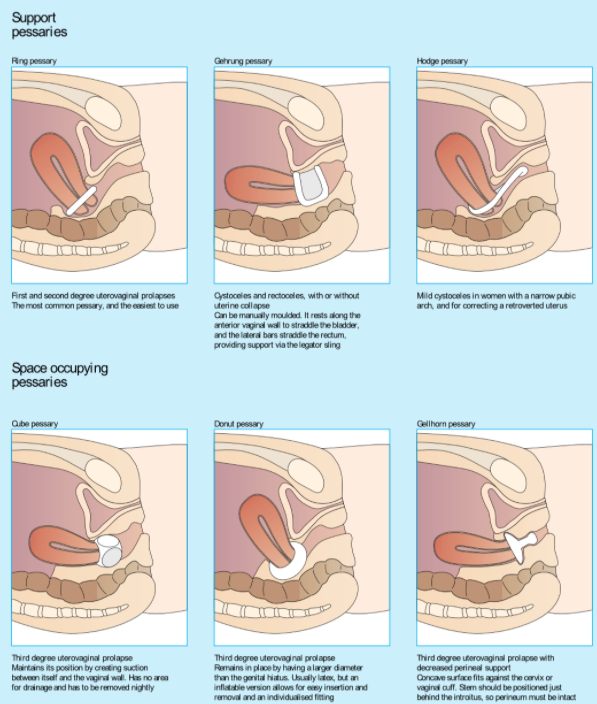
- Pessaries
- Surgical
- Mechanism
- Urge incontinence
- Sudden urge of urination followed by involuntary urinary leakage
- Urinary frequency and nocturia may also be described by the patient
- Causes
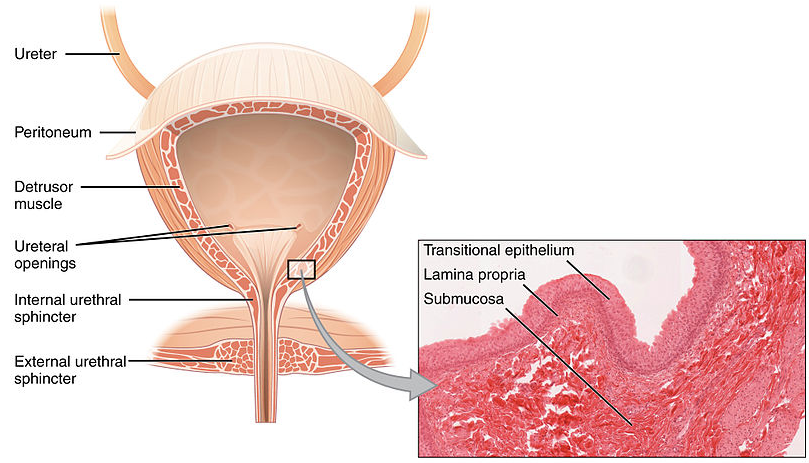
- Detrusor muscle hyperactivity
- Mechanisms
- Oftentimes idiopathic
- Commonly due to nerve or muscle damage
- Overflow incontinence
- Continuous slow flow of urine all the time or some time after urination
- Causes
- The bladder is always full and the ureteric flow is turning into urinary incontinence
- Mechanisms
- Insufficient emptying by the detrusor muscle, leading to a mostly full bladder
- Outflow obstruction (urethra obstruction) can once again lead to a full bladder and result in a constant dribble
- Mixed incontinence
- Stress and urge continence occurring together
- Transient incontinence
- Caused by issues that go away after a period of time
- UTIs, severe constipation, medications, etc.
- Functional incontinence
- The genitourinary system is working normally
- The patient doesn't make it to the toilet in time due to confusion, dementia, mobility or vision problems
All information provided on this website is for educational purposes and does not constitute any medical advice. Please speak to you doctor before changing your diet, activity or medications.
